Blog

Blog
June 19, 2024
Witnessing the Human Impact of Digital Therapeutics
by Nicholas Samendinger
Director of Brand, Creative & Design at Magic Leap
Blog
June 19, 2024
Witnessing the Human Impact of Digital Therapeutics
by Nicholas Samendinger
Director of Brand, Creative & Design at Magic Leap

Blog
June 17, 2024
Revolutionizing Construction: How Argyle and Magic Leap Are Transforming Architecture, Engineering, and Construction
All blogs
Blog
June 19, 2024
Witnessing the Human Impact of Digital Therapeutics
Blog
June 17, 2024
Revolutionizing Construction: How Argyle and Magic Leap Are Transforming Architecture, Engineering, and Construction

Blog
June 17, 2024
Delivering on the Promise of Technology: How Magic Leap and Strolll are Transforming Parkinson’s Care

Blog
April 22, 2024
Improve Precision and Efficiency with Magic Leap 2 for AEC
Blog
April 2, 2024
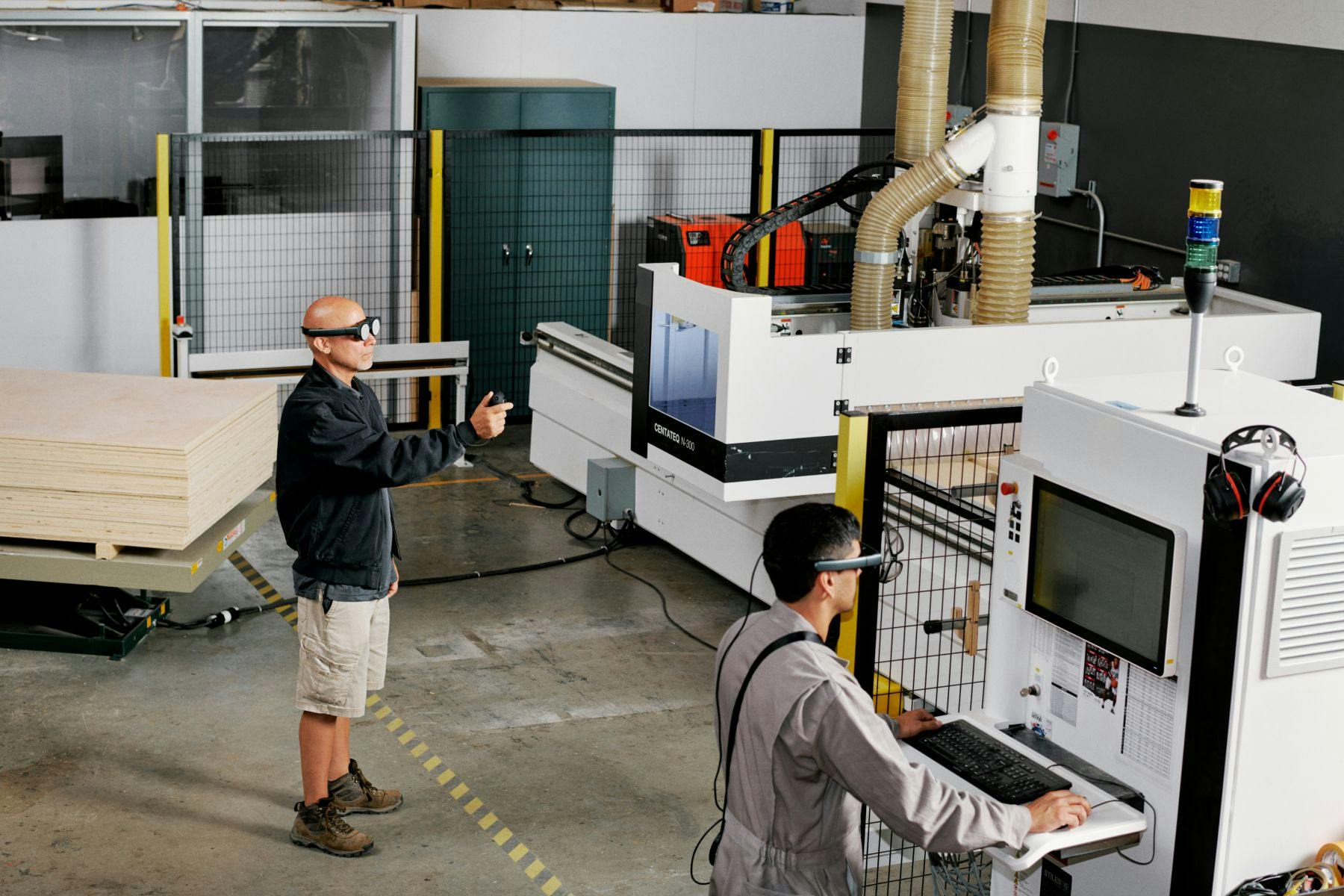
Enhance Manufacturing Productivity and Operational Excellence with Magic Leap 2

Blog
March 22, 2024
New Features on Magic Leap 2 Empower Developers and Enhance Enterprise AR Solutions

Blog
March 14, 2024
Enhancing Design Visualization for AEC: How HUSH Transforms Design Visualizations Using AR

Blog
February 3, 2023
Augmented Reality 101: What is AR and How Does it Work?

Blog
January 24, 2023
Augmented Reality 101: An Overview of AR for Business Leaders

Blog
August 30, 2022